

Whiplash and Whiplash-associated Disorder (WAD)
What is Whiplash?
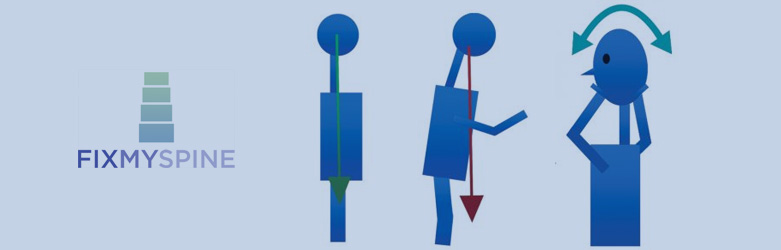
“Whiplash” refers to an injury involving the neck, when it has been subjected to a sudden flexion and extension mechanism. If a sudden forward-directed force is applied to a seat with an unsupported neck, the body accelerates suddenly forward, while the neck lags behind,causing the neck to extend. When the force stops, the body decelerates and the 3Kg weight of the head causes the neck to “overshoot” the body, resulting in excessive flexion. This sequence of motion is seen in a whip being cracked, but the effect can be exaggerated in humans because of the additional forces created by the head.
Whilst the original description of whiplash was in relation to the whip-like mechanism of an injury, there has been creepage, so that today the term “whiplash” is used to describe the neck pain experienced with a low velocity impact, typically a rear-shunt when driving a car.
Some people try to clarify the meaning of whiplash by describing either a “whiplash trauma”, which is the mechanism of an event, or else “whiplash injury” which relates to symptoms as a result of a whiplash trauma. To make life more complicated, a term called WAD or whiplash associated disorder is also frequently used to describe whiplash injury and these terms are used interchangeably.
Put simply: whiplash= whiplash injury= whiplash associated disorder= WAD= symptoms.
Whiplash trauma= the mechanism of a whiplash event.
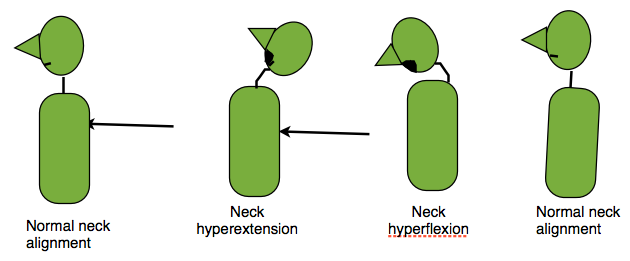
The acceleration-deceleration effect on the neck
a force pushing the body forward results in the neck initially lagging behind in extension, then the weight of the head catches up and overshoots the body, causing the neck to flex. The alignment of the head, neck and body are then restored.
What is Whiplash-Associated Disorder, or WAD?
This is a term used interchangeably with whiplash and relates to symptoms associated with a whiplash mechanism of injury.
Medicalising Whiplash
Since whiplash has entered the medical literature, more and more people involved in traffic accidents have successfully claimed compensation for whiplash injuries. The whiplash industry is now enormous in the UK, as outlined in a BBC news article in November 2015 http://www.bbc.co.uk/news/magazine-34925933. Unfortunately, the large numbers of people affected by whiplash, without an objective diagnosis to support the claim, means that some people involved in road traffic accidents may falsely claim for a whiplash injury and feign their symptoms in order to receive financial compensation.
The amount of litigation involved with whiplash has caused international concern in Western countries, with two investigations conducted in order to try and give whiplash some objectivity. The investigations have been funded by the motor industry in Canada and insurance companies in Sweden.
Both investigations gave reports to recommend that research was needed in order to gain a better understanding of the whiplash injury, but inroads were made to at least publicise a common language for terminology, so that research communication would be clearer in the future.
Canadian and Swedish Taskforce findings for Whiplash
There were two major publications published in relation to defining whiplash as an injury, the first from Quebec (1995) , financed by the motor industry, which looked at whiplash-associated disorders and the second from Sweden looking specifically at whiplash, initiated by four insurance companies. Both task forces tried to make neck pain and associated symptoms an objective disease entity, rather than a tool by which people can claim compensation following motor vehicle accidents.
The Quebec taskforce document is over 70 pages long and in summary, it tells us the following:
1 Whiplash is not a medical diagnosis. It is a description of an injury.
2 Most people who experience neck pain due to whiplash trauma recover quickly.
3 Neck pain as a symptom can be classified into four WAD (whiplash associated disorder) grades, which help estimate the recovery length of time (higher grade= longer recovery time)
0= no symptoms, nothing to find on examination
1= stiff, painful and tender neck, without anything to find on examination
2= neck symptoms and supporting restriction of movement along with point tenderness found on examination
3= neck symptoms and related nerve injury, such as weakness, numbness or loss of tendon reflexes, found on 00examination
4= neck symptoms and neck fracture or neck dislocation found on investigation.
Moving on to the Swedish task force’s publication in 2008; this report suggests that the term “whiplash trauma” should be used to describe the mechanism and “whiplash injury” should be used to describe the symptoms which result from the whiplash trauma. Whiplash injury and whiplash associated disorder (WAD) are terms which are used interchangeably and are therefore thought to describe the same type of symptoms. The report also suggests that the Quebec WAD groups 0 and 4 should be removed, since 0 represents no injury and 4 represents definable and easily diagnosed trauma, as evidenced by X Ray or CT tests.
Interestingly, the group found evidence to show that the symptoms relating to whiplash injury did not miraculously improve as soon as a legal claim was settled, implying that most people suffering with whiplash injuries are genuinely suffering with problems, instead of possibly feigning symptoms for financial compensation.
The commonest symptoms relating to whiplash injuries are reported as follows-
- Neck stiffness (96%),
- Neck pain (94%),
- Headache (44%),
- Pain between the shoulder blades (35%),
- Sleeping problems (35%),
- Signs of stress (30%),
- Numbess or pins and needles/parasthesiae (22%),
- Vertigo (15%),
- Memory problems (15%),
- Hearing symptoms- hearing test recommended- (13%)
- Eye symptoms (12%).
A common reason for the vertigo symptoms encountered with a whiplash trauma is due to displacement of otoliths within the middle ear, which causes benign positional vertigo. A test whereby the patient is quickly moved from a sitting to lying position (Dix-Hall-Pike test) causes the vertigo symptoms, usually accompanied by rapid eye movements called nystagmus. This symptom can be treated by the Epley monoeuvre, which aims to reposition the otoliths back where they belong in the middle ear and in doing this, cure the vertigo.
Prognostically, the longterm outcome of whiplash injury is usually very good, with most symptoms clearing up rapidly over days to weeks, but an estimated 5-10% of people have ongoing problems affecting their working lives. It is generally believed that if symptoms persist beyond two months, then they are likely to remain to some extent in the long term (there are reports of people’s symptoms improving over four years following a whiplash trauma, however). People who have severe neck pain initially also tend to develop chronic symptoms. There is a relationship between the WAD grade and time taken to recover from a whiplash injury.
Rest versus Exercise debate
The evidence points toward targeted exercise with regular supervision, instead of home-based exercise. The amount of exercise can gradually be increased as symptoms improve and can be helped along with simple over-the-counter painkillers.
Treatment is based on the symptoms, rather than a defined diagnosis, such as facet joint pain, or ligament strain, since these types of injuries are rarely detected on imaging including CT and MRI.
What are the risk factors for developing Whiplash symptoms?
1. The head rest.
One risk factor is related to the head rest position. If the neck is unsupported, then it is able to extend more than if the head were resting against a head rest. If the stiffness of the seat is different to the stiffness of the headrest, then the load-transfer will not be equal when a force is applied to the seat, even when the head and body are both in good alignment and both supported. It’s worthwhile making sure that both the height of the headrest and the inclination are correct so that the body is in a normal alignment when sitting.
2. Car bodywork design
The next risk factor is related to the rigidity of the car bodywork. Ideally, the car should have as much shock-absorption in the front and rear as possible, in order to minimise movement of the car when an impact occurs. A decent crumple zone for a car is bad news for the car’s bodywork, but good news for the car’s occupants.
3. Medical risk factors
Unfortunately, people who are already suffering with neck pain, or conditions which can cause neck pain such as rheumatoid disease, are more likely to suffer with a whiplash injury following a rear-shunt car accident. Also, people who are prone to anxiety or depression are also at risk.
Fairground rides and bumper cars
Bumper cars in fairgrounds typically reach speeds of 5mph. There are no headrests in dodgems and the seatbelts are nowhere as sophisticated as those fitted in a standard road-going automobile. Although most bumps may be anticipated and therefore, the occupants may brace themselves and arguably protect their necks, many bumps are surprise impacts. There is a single published successful lawsuit for whiplash following a head-on (not rear-shunt) collision with a dodgem in a fairground http://www.independent.ie/irish-news/courts/woman-wins-7000-for-dodgem-whiplash-26551477.html and now, fairgrounds are litigation-aware, posting “no bumping” signs on the bumper cars and also directing traffic flow to minimise collisions.
Unfortunately, the correlation between ongoing neck symptoms and the forces imparted during a collision is not available and this lack of information may explain why the rear-shunt dodgem population does not significantly feature as a group of whiplash sufferers, since the energy imparted with an impact may be lower than when motor vehicles are involved.
A prize-winning research article published in 1997 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3467723/pdf/586_2005_Article_BF01834062.pdf proved that at low speeds, there is no mechanical difference between a rear-shunt car accident and a rear-shunt dodgem collision, with evidence to show that there is more neck movement with a dodgem collision compared with a car collision. The paper could not address an important contributing factor with road traffic accidents, however, ie the stress and anxiety of being involved in a road traffic accident, as opposed to the adrenaline rush of enjoying a bump in a fairground dodgem ride (the dodgem driver has chosen to engage in a ride with a near-certain collision).
Many people involved in car accidents develop long term psychologic disturbance as a result of being involved in a car accident, rather than other reasons. There is plenty of evidence to show that people with depression or anxiety recover less well than those without psychological problems, not just with whiplash, but virtually any injury with a risk of longterm pain.
What about the Alar Ligaments in the neck- does damage to these cause the chronic pain of Whiplash symptoms?
There is convincing evidence to suggest that the alar ligaments at the very top of the neck bear the brunt of the force imparted on the neck during a whiplash trauma. Some researchers have demonstrated the ligament being injured on MRI. The clinical evidence is controversial,however, due to disagreement with interpreting the MRIs. The mathematical modeling data presents an attractive hypothesis for why some people develop longterm neck pain as well as headaches (http://ac.els-cdn.com.libezproxy.open.ac.uk/S0021929012000371/1-s2.0-S0021929012000371-main.pdf?_tid=d5f773a4-ada3-11e5-8766-00000aacb361&acdnat=1451335668_7946b99163f315197642db5da001f3a9). The alar ligament is a very strong pair of ligaments which help to attach the neck to the base of the skull. The ligaments are not easy to spot on MRI and often require specialised types of MRI imaging to assess the ligaments in detail. Even with close scrutiny of the ligaments, however, there can be disagreement in opinion (known as low interobserver reliability) when assessing the same MRI images of the alar ligaments
Whiplash in Summary
So, in summary, whiplash is a term used interchangeably with whiplash-associated-disorder (WAD) and is used to define the injury caused by a whiplash trauma. The whiplash trauma is an acceleration-deceleration mechanism in one direction, usually involving a motor vehicle rear-shunting another motor vehicle at low velocities. Most people involved in a whiplash trauma experience short-lived neck stiffness and pain, with a minority of people going on to develop long-term symptoms. There are no specific tests which can prove a whiplash injury and there is no evidence to show that resting the neck helps the situation. On the other hand, there is evidence to show that supervised exercise following a detailed clinical evaluation tends to improve the rate of recovery. For those people who develop vertigo as part of the whiplash injury, the symptom can possibly be easily remedied by a corrective manoeuvre called the Epley manoeuvre. A hearing test is recommended if hearing problems are experienced with a whiplash injury. Any psychologic issues experienced due to a whiplash trauma should be treated in conjunction with the pain or physical disability experienced.
Finally, all are in agreement that there is a lot of research needed to try and understand why so many people suffer with whiplash injuries following seemingly minor road traffic accidents, in a bit to reduce the burden of suffering, as well as reduce the economic implications of employment, medical treatment, insurance premiums and litigation.
Exercise for Whiplash symptoms
The evidence directs us away from resting the neck and toward supervised exercise. The injured person needs to be assessed by a medical expert in the first instance, in order to make sure that there are no injures requiring further investigation and that it is safe to proceed with exercises. There is no evidence to show that either rest of neck supports help recovery from a whiplash injury.
There are many different health professionals who offer help with whiplash-related pain, including chiropracters, osteopaths and physiotherapists. It appears that the best recovery is achieved when the person suffering with pain relates well with a single health professional and has continuity of care while following a prescribed exercise regime.
Pain-relieving medication for Whiplash symptoms
Pain killers can be either taken by mouth as medications, or applied to the painful area topically.
For tablet painkillers, firstly, make sure that you are able to take any type of painkiller. Some people with asthma cannot take anti-inflammatories, or NSAIDs, for example, as well as people with a history of stomach ulcers or advanced kidney disease.
Most people can use paracetamol as a basic pain killer. Taken regularly at the recommended dosage as stated on the packaging, this medication can be effective for mild to moderate pain. If more pain relief is needed, then a low dose morphine-based tablet such as codeine phosphate could be added to the paracetamol, but be aware of constipation as a common side effect of morphine-based medication. A non-steroidal anti-inflammatory such as ibuprofen could also be added to both the paracetamol and codeine for treating moderate to severe pain in the short term. If you feel that all three types of pain killers are required to try and control your pain, you should discuss this with your GP.
As a rule of thumb, pain can be scored on a scale from 0 to 10. This is called a visual analogue score, or VAS. 0 represents zero pain and 10 represents the worst pain imaginable. In general, a VAS of 7 and upwards is regarded as severe pain and this should be addressed by a doctor.
Danger signs for whiplash
This is not an comprehensive list of symptoms that require medical attention and if you are concerned about any symptoms relating to a whiplash injury, you should seek medical help from your doctor.
1 Arm/hand or leg/foot weakness
2 Uncoordinated walking/ unsteady walking
3 Clumsy hands, loss of dexterity, dropping objects, loss of ability to fasten buttons
4 Progressive numbness or pins and needles ie either spreading distribution or increasing intensity
5 Increasingly severe neck pain
6 “Heavy head” ie feel the need to physically hold the head as it feels to heavy to hold up