

Do your legs get tired and heavy when you walk
Do your legs get tired and heavy when you walk?
Then you’re not alone.
Many people suffer with their legs, which can stop them going out for that refreshing coastal walk. It’s quite debilitating.
Limited walking distance due to tired legs is typically described as claudication, which derives from the Latin word claudus, meaning “lame”. In medical terms, claudication relates to limited walking distance due to either a circulation/vascular problem (vascular claudication) or a spinal problem (neurogenic claudication). It’s possible that both problems can co-exist, of course, but vascular claudication pain tends to ease when you stand still, allowing the circulation to wash away the build up of lactic acid which has built up in the muscles through walking. On the other hand, neurogenic claudication tends to ease when you sit down, leaning forward to create a little more space for the compressed nerves in the spine.
With neurogenic claudication, the walking distance can be improved by commandeering a shopping trolley when picking up the groceries. The act of leaning forward can considerably improve the walking stamina and delay that increasing feeling of leg heaviness, like wading in mud. Some people experience sciatica symptoms which quickly resolve after a few minutes of sitting down, so that they look for benches to rest on when walking from point A to point B.
Neurogenic claudication is due to a condition called spinal stenosis (“stenos” is Greek for “narrow”). Nobody knows for sure why some people develop narrowing in the spine, but the condition usually evolves over a number of years, with symptoms gradually developing over time.
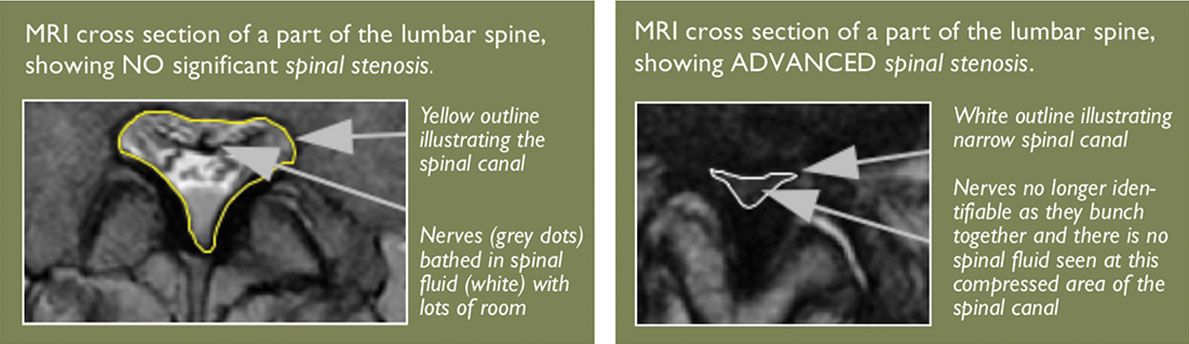
A health professional can help to diagnose spinal stenosis, matching the symptoms of neurogenic claudicationand examination findings which tend to be fairly innocuous, with the MRI appearance of a narrowed spinal canal. Getting the right information together in order to suspect spinal stenosis isn’t as easy as it sounds. Health professionals tend to take a history and examine people differently, so a group of researchers organised a huge survey of 279 different health professionals from 29 different countries to find out if they could agree on questions which were most likely to point to the diagnosis of spinal stenosis. 80% of them agreed on the following:
1. Leg or buttock pain when walking
2. Bending forward to relieve symptoms
3. Feel better when using a shopping trolley or a push bike
4. Weakness, heaviness, numbness, tingling in legs when walking (motor or sensory disturbance
5. Equal and normal pulses in the feet
6. Weak legs
7. Low back pain
These 7 questions were found to be so useful that the paper reporting these findings in August 2016 was awarded a prize by the International Society for the Study of the Lumbar Spine (ISSLS). When a health professional suspects neurogenic claudication (symptom), the diagnosis of spinal stenosis is made by MRI.
Things to do to try and help improved your legs
1. Exercise
There is evidence to show that doing exercise such as aquatic walking ie. walking in a swimming pool helps to improve the symptoms of spinal stenosis.
2. Lose some weight
Weight loss may also help to improve symptoms of neurogenic claudication, with some researchers suggesting that the act of offloading the weight on the spine by leaning on a shopping trolley is the reason why people can walk for longer with spinal stenosis. There is also an association between body mass index, or BMI, and the development of symptoms in association with spinal stenosis.
3. Spinal surgery?
When exercise and walking aids, such as a rollator, don’t go far enough to improve the symptoms of spinal stenosis, then surgery can be considered. The commonest operation for spinal stenosis is called a lumbar decompression operation and it is one of the commonest procedures performed by spinal surgeons. This is hardly surprising, when researchers estimate that 9% of the population over 65 years old has spinal stenosis on MRI.
The British Association of Spinal Surgeons has produced useful information about both spinal stenosis and lumbar decompression surgery, with the website details cited in the references at the end of this article. In essence, a lumbar decompression operation involves removing excess tissue which is causing the narrowing in the spinal canal, to allow more room for the spinal nerves. Spinal surgery is not risk-free, however, with surgeons typically quoting an estimated risk of around 1:1000 that the operation may result in permanent paralysis.
Although surgery has a high chance of improving the symptoms of neurogenic claudication, the evidence is not as convincing as perhaps we would like it to be. In 2016, a Cochrane review of published evidence showed a preference for surgery over non-operative treatment, but the authors raised concern over the lack of strong evidence to support surgery. On the other hand, the authors reported the complications recorded in the study such as wound infection, but there were no reported complications in association with treatment that did not involve surgery. The authors recommended caution when recommending surgery due to their findings.
In summary, if you can’t walk as far as you would like to, due to your back and legs becoming painful, heavy and weak, then you may have symptoms of claudication. It’s worth seeing your GP in order to establish a firm diagnosis and then you can try getting your weight into the normal range for your height e.g. around ten stones if you are 5 foot six inches tall and exercise more. If this doesn’t help, sometimes, a spinal decompression operation can help to improve your symptoms. References supporting this article and further reading (most of these are free downloads online).
7. Lumbar decompression surgery. British Association of Spinal Surgeons website www.spinesurgeons.ac.uk/patients/patient-information/lumbar-discectomy-and-decompression accessed July 24th 2016.
8. Surgical versus non-surgical treatment for lumbar spinal stenosis (Review). Zaina et al. Cochrane Database of Systematic Reviews 2016, issue 1.
9. SPINE Volume 41, Number 15, pp 1239–1246ISSLS Prize Winner: Consensus on the Clinical Diagnosis of Lumbar Spinal Stenosis results of an International Delphi Study. Christy Tomkins-Lane et al.
Text Neck
We ignore the influence that our 5Kg heads have on our unsupported necks as we constantly hold our heads in front of our body by bending our necks
 Standing upright with good spinal posture, results in the weight of our body, from our head downward, being transmitted very close to the spinal column. The shock-absorbing discs are loaded symmetrically and are therefore less likely to wear out. The green arrow represents our ideal “centre of gravity”.
Standing upright with good spinal posture, results in the weight of our body, from our head downward, being transmitted very close to the spinal column. The shock-absorbing discs are loaded symmetrically and are therefore less likely to wear out. The green arrow represents our ideal “centre of gravity”.
 Looking down brings the head forward in relation to the body. This means that the 5Kg weight of our head is generating a centre of gravity which runs in front of the spine. The shock-absorbing discs are now eccentrically, or asymmetrically loaded. This means that there is more force going into the backs of the discs rather than the fronts of the discs and, over time, the discs fatigue, fail and bulge backwards. The red arrow represents the “centre of gravity”.
Looking down brings the head forward in relation to the body. This means that the 5Kg weight of our head is generating a centre of gravity which runs in front of the spine. The shock-absorbing discs are now eccentrically, or asymmetrically loaded. This means that there is more force going into the backs of the discs rather than the fronts of the discs and, over time, the discs fatigue, fail and bulge backwards. The red arrow represents the “centre of gravity”.
Our shock-absorbing discs have to put up with eccentric pressure placed upon them, which, like a repetitive strain injury, gradually wears the back of the discs and causes them to bulge. When we start experiencing neck pain or pins and needles in our hands, then this can be the first sign of a problem which we generated when we first started attending to our smart phones a few years ago.
Here’s some supporting evidence
A Japanese study in 2016 reported that people with weak muscles at the back of their neck also suffer with trapped nerves in the neck. This suggests that habitually bending the neck forward and neglecting neck extension results in the tendency for spinal nerves in the neck to become pinched, usually by disc bulges. While the MRI evidence appears very convincing to those who understand the biomechanics of how discs wear, it could be argued that the MRI is a snapshot in time, so it’s impossible to prove cause and effect from the same picture. True, but, a second publication from 2008 linked poor neck posture with more wear in discs in the neck. Another article in 2002 showed reversibility of disc bulges on MRI by placing people’s neck in traction and hey presto, the disc bulge went away while the traction was in place.
Here’s a simple test (look around and make sure that nobody’s watching you).
 Step 1. Look up to the ceiling
Step 1. Look up to the ceiling
Step 2. Look down to the ground
Step 3. Put this lovely magazine down, and put one hand on the back of your head and the other hand on your chin
Step 4. Now repeat step 1 and step 2
You will find that in order to look up and look down, you have nodded your head.
You have not, however, moved your neck.
Over time, our habitual neglect of neck movement in preference of head movement means that we allow our necks to stiffen up, as well as habitually overload our discs in our necks by holding our head too far forward in relation to the rest of our body.
 See for yourself: Here are X Rays used to looking at neck mobility in somebody who was asked specifically to look up as far as possible and down as far as possible.
See for yourself: Here are X Rays used to looking at neck mobility in somebody who was asked specifically to look up as far as possible and down as far as possible.
While the skull is moving well at the top of the neck, the neck itself hardly moves at all!
So, what can we do to prevent neck problems due to “wear and tear” or spondylosis?
Robin McKenzie, a physiotherapist from New Zealand, understood the importance of good posture and maintaining spinal flexibility. In his book “Treat Your Own Neck”, he demonstrated a series of neck extension exercises which he and many others have found beneficial in relieving neck pain. Although exercises are useful, ideally, we should be habitually and constantly checking ourselves to make sure that we are not drifting into slouched, spinally-challenging postures. We should give ourselves a spinal stretch now and again, by arching our necks and our backs backwards ie. the opposite of the slouched posture, in a bid to stop our spines from stiffening up.
Next year, make the most of gazing at the sky when the Air Show comes to town and, until then, raise your arms when texting to maintain a horizontal gaze. This way, you should avoid the growing trend of neck pain due to “Text Neck”.
Dynamic Sitting? Tell me more…

“Balancing” courtesy of Pixabay images
How many of us are bothered with back pain, especially when we sit down for a long time? Lower back pain is inevitable if your body posture is not ideal while sitting down for long periods. There is an abundance of published evidence pointing to the detrimental effects of sitting with a slouched posture, as well as staying in one position for long periods of time. A study in the European Spine Journal (Liss 2007) showed that while prolonged sitting is bad, prolonged sitting in an awkward posture is even worse for the back. We have a tendency to adopt fixed and awkward postures when we drive a car, for example, with driving not only giving us back pain, but it also increases the risk of gaining excessive weight and developing heart problems.
So is prolonged sitting is bad for us? In most cases it looks like it. While sitting avoidance may be fairly easy to achieve when deciding whether to walk to the corner shop versus driving there, (walking wins!) it’s less easy to avoid sitting when our jobs are desk-based. So how can we avoid spinal problems which result from prolonged sitting?
For a start, let’s look at the commute to work. If we can catch a bus instead of driving, we are more likely to walk to a bus stop and then walk to our destination when we get off a bus- this is called “active travel” instead of passive driving. Catching a bus is also good for the environment by reducing our collective carbon footprint.
But, how about the rest of us who can’t avoid sitting down for long periods of time? A team of researchers from Japan and Thailand recruited 74 volunteers aged between 18 and 25 years old and split them into two seated groups. One group sat and enjoyed a two hour movie while the other group watched the same film but repeated an exercise regime every 20 minutes. The people who exercised while sitting in (“dynamic sitting”) had significantly more flexible lower bags compared with the groups that stayed still.
So, the way to dynamically sit is as follows:
Step 1 Set a timer to alert you every 20 minutes for your active sitting session.
Step 2 Extend your lower back until you can feel a slight stretching in that area.
Step 3 Hold the back extension pose for about fifteen seconds
Step 4 Gently draw in the abdomen to return to the neutral sitting position over 15 seconds
Step 5 Repeat six times
In between the active sitting sessions, focus on sitting upright as tall as possible and facing downwards (see my previous article “text neck” to read why).
Happy Sitting!
Treating Whiplash the Osteopathic way
Many people who suffer from the pain of spinal injuries seek the help of osteopaths.
Osteopathy is a gentle and effective hands-on approach to healthcare, based on the principle that the way your body moves affects how it functions.
Osteopathic practitioners are state registered healthcare practitioners recognised by the NHS and capable of diagnosing and treating musculoskeletal (Muscles, bones and joints) problems independently. You do not need to see your GP prior to consulting an osteopath but in some cases the osteopath will refer you to your doctor if the nature of your problem requires medical treatment (www.osteopathy.org).
Evidence which reviewed scientific studies on the types of treatments used by osteopaths showed that these approaches were successful at helping to relieve the head and neck pain that often accompanies a whiplash injury (Gross et al,2002). The advantage of this gentle approach can mean that the patient is able to return to normal activities without surgery and with a reduced need to take medication.
A consultation with a registered osteopath will entail a full and detailed case history which will aim to get to the root of the problem. In addition to this the osteopath will perform detailed examination of your movements as well as clinical testing of the musculoskeletal and nervous systems as appropriate. Osteopathic treatment involves a range of techniques which focus on addressing dysfunctional changes in your body tissues which have resulted from excessive strain. These techniques will range from conventional soft tissue massage and manipulation to joint mobilisation and manipulation techniques which improve healthy movement of the muscles bones and joints. As a comprehensive approach to musculoskeletal pain and dysfunction osteopaths can also prescribe therapeutic exercise programmes which are tailored specifically for you and increase the benefits of the physical treatment they provide so as to get you back to a pain free state in the most effective and timely manner.
Many different structures are injured by whiplash. Due to the rapid extension (backward bending) of the neck during the initial stage of the injury the joints at the back of the neck are rapidly compressed. This can cause significant pain which lasts for a long time after the initial injury has subsided. In addition to this vulnerable nerves may be compressed as the forceful extension of the neck may pinch and bruise the sensitive roots of the nerves which exit the spine at the side of the neck. Many patients find that this is a cause of pain which travels down the arm after the initial injury has occurred. During the flexion phase of the whiplash injury the tissue at the back of the neck is stretched too quickly whilst during the extension phase of the neck the tissues at the front of the neck are stretched too quickly. This can result in painful muscle tears which cause swelling and inflammation as well as on-going spasm if they fail to heal optimally.
The effects of a whiplash injury can last for many months and sometimes years after the initial damage. This is in part due to the fact that the neck and spine is no longer moving in as natural and smooth a way as before. These changes make it harder for sufferers to withstand the stresses and strains of daily life such as housework, deskwork and moving objects. Interesting research (Weisberg 2000) also shows that the function of the muscles of the neck and jaw becomes disordered as the electromyographic (how the nerve sends impulses to the muscle) activity is altered. This pattern of muscular dysfunction can cause accelerated wear and tear on the delicate joints of the neck leading to arthritis and has also been shown to cause problems which increase the rate of age related wear and tear in the jaw joint (Garcia & Arrington 1996) which can lead to problems with eating and speaking later on.
After your osteopath has examined you they will typically use advanced soft tissue massage techniques to relax tight and painful muscles as well as gentle joint mobilisation and stretching to restore function to spinal joints which have stiffened up due to the trauma of the whiplash injury. Most often the osteopath will examine and treat joints in other parts of the spine such as the mid and lower back which due to their connection to the neck may be reacting to the initial injury. Depending on your individual case there may be issues such as previous injuries and existing problems with any of the body’s tissues which are aggravated by the whiplash injury. When this is the case your osteopath will treat these areas as well in order to reduce the cumulative strain on the whole body and allow you to move optimally and heal faster.
An important aspect of osteopathic treatment is to prescribe exercises which you can do between treatments. Rehabilitative exercises for whiplash injuries are aimed at improving function and reducing strain on the damaged areas of your spine. The osteopath will usually give these during the first or second treatment and will carefully monitor and adjust the exercise plan as your body changes with treatment. Depending on the extent of your whiplash injury the osteopath may need to see you a number of times however most patients with spinal pain find significant relief after 2-6 sessions.
(Garcia & Arrington 1996)The relationship between cervical whiplash and temporomandibular joint injuries: an MRI study. Cranio : the Journal of Craniomandibular Practice [1996, 14(3):233-239]
Gross et al 2002. Manual therapy for mechanical neck disorders: a systematic review. Manual Therapy. Volume 7, Issue 3, August 2002, Pages 131–149
Weisberg 2000. The craniocervical connection:A retrospective analysis of 300 whiplash patients with cervical and temporomandibular disorders. Cranio 18(3):163-167, 2000.
Why Does My Back Hurt? The Biomechanics of back pain explained
Your ‘backbone’ or spine comprises a series of separate bones (vertebrae) joined together by deformable intervertebral discs, which are tough gristle-like pads of cartilage. Adjacent vertebrae are also connected by small sliding joints, the apophyseal, or facet, joints (Figure 1), and by ligaments which are tough fibrous bands. All of these structures, including the discs, have nerves that are capable of signalling pain.
Unfortunately, the spine lies so deep in the body that it is difficult to put your finger directly on the pain source. However, several research studies have managed to do just this: the treating clinician has prodded and poked inside their patients’ back until their exact pain is reproduced. These heroic diagnostic studies, which sometimes involved expensive imaging techniques such as MRI, have shown that severe and chronic back pain most often comes from intervertebral discs, and from the apophyseal joints. Often, the MRI images reveal abnormalities in structures that turn out to be unrelated to the chronic pain! In contrast, back pain that flares up quickly and is gone in a week appears to come from overstretched back muscles or ligaments.
Because of the pain and expense of diagnostic tests, and because the tests are not 100% reliable, most clinicians do not use them with each individual patient. Instead they use information from the research studies to estimate where the pain is probably coming from in each patient. If they suspect there is no serious underlying problem, the clinician may perform no invasive tests, and simply refer to the patient as having ‘non-specific back pain’. This just means that the patient has back pain, that the pain is of unknown origin, and that it is expected to clear up quickly. It can be frustrating for the patient not to know precisely where their pain comes from, but uncertainty is often better than invasive and possibly misleading diagnostic tests.
A great deal of non-specific back pain is probably just ‘functional’ in the sense that it arises from the manner in which the patient uses their back, without there being any underlying injury or degeneration. For example, standing for long periods in a lordotic hollow-back posture can give rise to high compressive and shear forces being concentrated in the apophyseal joints (Figure 1), or in parts of the disc. This can cause backache for as long as the posture is maintained, but the pain soon fades when the patient adopts another posture, such as sitting.
Patients can also be frustrated if they are told (or otherwise find out) that there is a suspected ‘psycho-social’ component to their pain. But this does not mean that the pain is not real, or ‘all in the head’. It simply means that the clinician believes that aspects of the patient’s behaviour (such as the decision to seek treatment, or to report that they are feeling better, or not) are significantly influenced by psychological factors such as fear of injury, or by social factors such as a physically-demanding job. And why wouldn’t they be!
Clinicians must treat whole patients and not specific symptoms, and recognising the involvement of psycho-social factors may help to prevent inappropriate or unnecessary treatments.

Fig 1 This side view of the lumbar spine (lower back) shows five vertebrae, separated by intervertebral discs which are shaded blue. The surface of the back is shown on the right, in orange, and the region occupied by a typical apophyseal joint is shown by the red circle. S and C denote the direction of compressive and shear forces acting on the spine. Figure adapted from: “The Biomechanics of Back Pain” by Adams, Bogduk, Burton and Dolan. Publishers: Churchill Livingstone (3rd Edition 2013).